
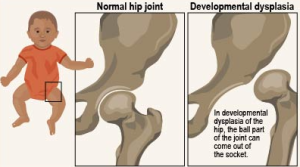
 DDH is a condition where the hip joint hasn’t formed correctly. In a healthy hip, the top of the thigh bone (femoral head) fits snugly into the socket of the pelvis (acetabulum). With DDH, this socket may be too shallow, or the femoral head may not be held firmly in place. This can range from the hip being slightly loose to the femoral head being completely dislocated from the socket.
DDH is a condition where the hip joint hasn’t formed correctly. In a healthy hip, the top of the thigh bone (femoral head) fits snugly into the socket of the pelvis (acetabulum). With DDH, this socket may be too shallow, or the femoral head may not be held firmly in place. This can range from the hip being slightly loose to the femoral head being completely dislocated from the socket.
It can affect one hip or both, and while it’s often present at birth, it can sometimes develop in the first few months or even years of life

